
Prevotella copri overgrowths

Author Bio
Absurd Prevotella overgrowths have been observed in many “sick” individuals and there is a high correlation to the overgrowth and exposure to moldy environments, meaning they have been found to be living in conditions where mold was discovered and or elevations on urine based mycotoxin tests. There are other situations and evidence trails that you must read about below to get a better understanding. Specifically the microbe found most overgrown is Prevotella copri in these situations.
Prevotella copri is a bacteria with substantial supporting evidence that it is fed by fungal metabolites and it is a surrogate for invasive fungal overgrowth - with high probability of mold exposure or harboring a fungal overgrowth driven dysbiosis.
A collection of literature snippets can be found here.
The rest of my argument is supported from clinical experience, situational changes, and testing. Having seen a higher than normal dysbiotic population than ASD, I would estimate this overgrowth is occurring in about 10 to 15% of individuals. Recently a paper was published recognizing this.
There is a lot of conflicting sources in this area, know that different eras of stools testing processed Prevotella as Bacteroides, in the 1990s the genus Prevotella was described by reclassifying a groups of Bacteroides, admittedly until recently even some stool testing has pooled Prevotella into the Bacteroides genus.
Thus it is impossible to know the full scope of the Prevotella issue unless you are using testing that follows NCBI classifications (likely the case for newer sequence based testing).
There are some infamous Biome researchers in ASD that will not recognize this Prevotella issue because it is in opposition to research they did decades ago, however I’m delighted that it is being recognized in recent publications. One famous FMT physician guru wrote my concerns off as it being completely from the diet despite being unable to explain why an 8 month old had it occupying 50% of their biome or the sudden changes in levels following the administration of an antifungal.
The overgrowth when present ranges from 20% to 90% of the entire microbiome (percentage abundance), certainly the distribution in the broad population looks very striking for this microbe and some other Prevotella.
The majority of samples in the broad population have percentage abundance well below a half percent abundance, and there is a sudden and sharp rise in the percentage abundance in the broad population somewhere around the 80th percentile.
It has been found elevated in multiple family members - all experiencing varying levels of illness.
This statement means that in a house of 3 or 4 people, often times when one individual is occupied with this excessive abundance, there is at least one other individual with the overgrowth present.
It has been found in an 8-month old child - where the mother had elevated levels as well, the child is not on solids.
It has been found in a 18-month old child where there were clear pictures identifiable of mold growing in the home.
There have been several situations where the microbe was NOT elevated on a first test, then the individual took some kind of intervention (probiotic, or antifungal, or FMT) and a subsequent test showed exceeding high levels (occupying 50% or more of the biome).
Most people that intervene see an increase in their percentage abundance on their next test but also report improvement.
This microbe / overgrowth does not respond in the same way that other microbes do to intervention, it appears to increase at first, given the behavior that it is feeding on some fungal metabolites (supported by literature).
It is elevated in different diseases HIV, RA, PA, all with fungal undertones.
It has been found to significantly diminish in the presence of Montelukast only for the duration of taking it and then quickly blooming back. There is a hypothesis there may be a viral3 tone, recently it was discovered that a bacterial virus inhabits certain Prevotella copri. Monetlukast is known to have an antiviral action, there are several components which seem to have efficacy in reducing the apparent overgrowth. Vitamin A, Perilla, Bacopa, Boswellia, Codonopsis, Olive leaf. Many of these also have action counteracting leukotrienes.
There are certainly different strains of Prevotella copri, this likely plays some role.
There appears to be a feeding mechanism that may over-exaggerate the overgrowth possibly in the distal colon.
It is possible that the level of the percentage abundance of Prevotella copri seen in stool tests is not reflective of the actual value inside the body. I believe that fungal metabolites are released in the wake of killing fungi or possibly as a threat of mycotoxins in response to antifungal intervention (Look up Neil Nathan) causing artificial blooms of this microbe to feed on the metabolites just as long as they are present in the colon.
I have attempted to measure a time lag effect, taking the same stool sample and evenly dispensing it amongst two vials and sending them for processing at distinct times. The result showed that there is a high variability in the P copri percentage abundance but also seeming to indicate that older samples caused feeding in the sample on metabolites which produced larger percentage abundances.
The result of all this is simply that the value of Prevotella copri is actually not very important if you are dealing with an elevated situation as I’m describing. Instead take it as a surrogate for a challenging situation where there is likely a large fungal issue and possibly a viral issue as well.
There is a counterargument that diet reflects high values of Prevotella copri consistent with certain geographical or cultural situations, certainly these high levels that I’m speaking about are not indicative of those diets (Mediterranean for instance), with almost all of the individuals I have worked with not even having a diet that resembles this at all, certainly this is the cases of the infants who have not begun solids. The distinct behavior of huge increase in P. copri abundance with antifungal components along with the supporting literature for this microbe feeding on fungal metabolites speaks volumes. There are also many cultures where fungal issues have recently been identified to be lurking in the dark, for instance India1.
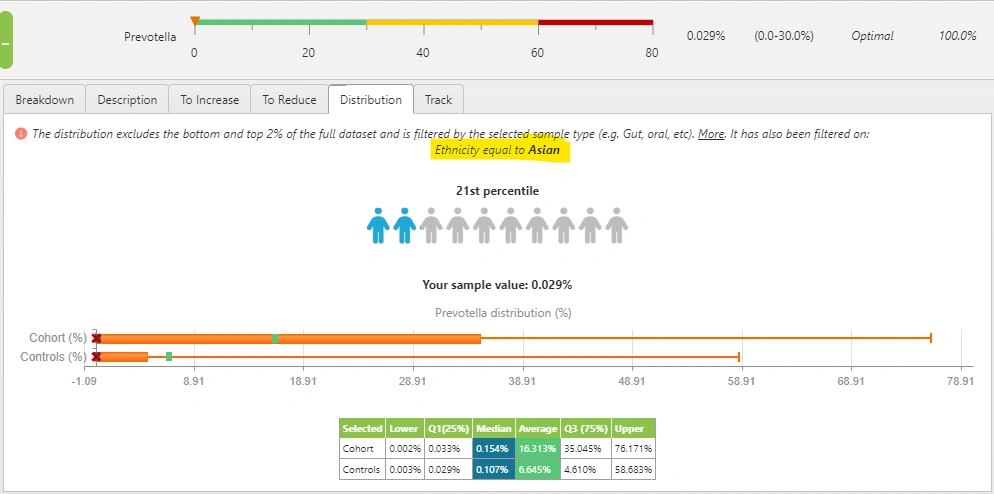
Using the Biomesight cohort selector, we can see the difference in Prevotalla abundance between Asians and the rest of the population. We can see the middle 50% is 0.033%-35% amongst Asians while in the general population it is 0.029% to 4.6%.
One could make the argument that mycotoxins in foods and the role they play with regard to cultural diets may play a role for the metabolites driving P. copri dysbiosis, a colonization in the GI tract is also possible. Yeast species such as candida are known to take on colony-forming mold like behaviors when exposed to more alkaline environments and have also been known to secrete mycotoxins.
It is also useful to note that DON toxin (Deoxynivalenol) aka VOMITOXIN is one that is not readily measured on mycotoxin testing and may be the most ubiquitous mycotoxin. There is some evidence that P. copri also metabolizes this toxin.
One way to determine if a mold or mycotoxin generating fungal colonization exists is to perform mycotoxin testing before the administration of an antifungal and shortly thereafter in the wake of the therapeutic, rise in oxalates and mycotoxins like Gliotoxin (often orders of magnitude) occur in response to antifungal regimens. This is well described by Neil Nathan and I have witnessed this. If no appreciable rises are measured then likely the source of mycotoxins is food-driven and or poor detoxification status or both. Regardless, the approach to healing should be the same as outlined above, substantial support for pathways, histamine-assisting tools, and potentially binders as needed, all while seeking to rebalance the gut.
Individuals that are battling oxidative stress and or mycotoxins can explore the lotion from Thiogenics which assists in the recycling of glutathione. There have been some nice messages left by those with ASD in response to trialing this product.
Elevations in Prevotella: Both fungal and viral implicated. Prevotella overgrowths occupying double digits certainly align with fungally fed situations. Best tools for these overgrowths: Codonopsis, Ashwagandha, Perilla, Vitamin A, Bacopa, Boswellia, Olive leaf, L Johnsonii, Rosemary, Curcumin, Ginger. Introduce antifungal components. AZ2 probiotic and support for fungal overgrowth which can include a light biofilm enzyme given on alternative days like candex for the 6 week duration at least.
References
- Animesh Ray, Adarsh Aayilliath K, Sayantan Banerjee, Arunaloke Chakrabarti, and David W Denning. Burden of Serious Fungal Infections in India
- Nehal Adel Abdelsalam, Shaimaa M. Hegazy & Ramy K. Aziz (2023) The curious case of Prevotella copri, Gut Microbes, 15:2, DOI: 10.1080/19490976.2023.2249152
- New, giant bacterial virus found in human gut
Categories: prevotella Tags: prevotella